Background
Cornwall and the Isles of Scilly received over €1 billion in EU funding from 2000 to 2020, including Objective One status, because its GDP was below 75% of the EU average, making it one of the poorest regions in Northern Europe.
Following Brexit, they were allocated £186 million to spend on local investment through the Shared Prosperity Fund. This funding runs out at the end of March. Cornwall got nothing in the recent “Pride in Place” handouts that mostly went to urban areas.
Cornish identity plays a big role – but is it backed up by science?
In 2014 “The Cornish” were recognised as a national minority under the European Framework Convention for the Protection of National Minorities, the same status as other Celtic communities the Scots, Welsh and Irish.
On the question of “Cornish Identity” Owl’s scientific correspondent has some interesting observations to make. The science doesn’t fit comfortably with this idea.
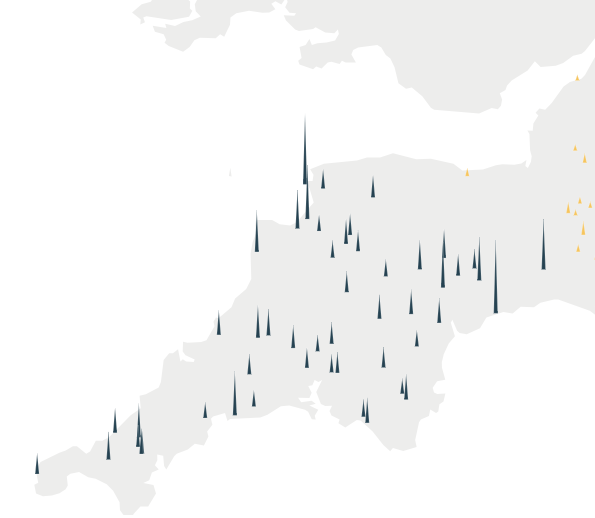
A paper published in “Nature” in 2015 examined the fine-scale genetic structure of the British population. What this examination showed was that those of deep Cornish heritage did form a distinct genetic subgroup in Britain. But it also showed that those with deep Devonian heritage also formed their own distinctive subgroup. Furthermore, only these two counties, Devon and Cornwall, in England had distinctive populations that mapped the county boundaries. Other genetic groupings were more widely distributed with some significant overlapping as well.
The genetic differences between Cornwall and Devon are comparable to those between islands in Orkney.
The ancestry profile of Cornwall is quite different from that of the Welsh clusters and is much closer to that of Devon and Central/Southern England.
The authors argue more generally that in non-Saxon parts of the United Kingdom, there exist genetically differentiated subgroups rather than a general ‘Celtic’ population.
Now throw into the mix the strict hierarchical rules that Labour is sticking to in its local government reorganisation plan such as: full devolution powers only go to strategic mayoral authorities (SMA); and SMA must preside over two or more unitary authorities.
Owl has sympathy with the Cornish cousins. We aren’t really that different.
Is Cornwall about to lose its independence bid?
The long-running campaign for Cornish devolution has been brought sharply into focus by the Labour government’s plans to decentralise power from Westminster. But Cornwall wants devolution without being forced into a marriage with Devon.
Martyn Oates www.bbc.co.uk South West political editor
Cornwall celebrated St Piran’s Day earlier this month. At Westminster, it was marked by a debate led by Camborne and Redruth Labour MP Perran Moon.
Events to mark St Piran’s Day are not unusual in parliament. Neither was a call Moon made for the devolution of “bold, flexible and meaningful powers” to Cornwall.
However, his call also fired a shot across the government’s bows just weeks before the Devolution and Community Empowerment Bill is expected to become law.
The campaign for Cornish devolution has been ongoing for decades. The actual process began just over 10 years ago when it was the first rural area in the country to be granted a “devolution deal” in 2015.
In 2023, Cornwall Council negotiated an upgrade to a “Level 2” deal, external with Rishi Sunak’s government, later ratified under Labour.
Cornwall’s established enthusiasm for devolution seems, at first sight, a perfect fit with this government’s determination to roll out “devolution by default” nationally.
But conditions minsters are imposing are problematic for many.
So, what are the problems?
One is the government’s insistence the basic unit for devolution should be two or more unitary authorities (all councils are soon expected to be unitary under government plans) grouped together, becoming a strategic authority.
Cornwall being forced to form a larger unit with Plymouth, Devon or anywhere else is anathema to the majority of Cornwall’s elected politicians, whose red line is devolved powers should be exercised by Cornwall alone.
Ministers also insist the highest level of devolved powers over things, such as planning, will only be granted to areas which accept a directly-elected mayor, who leads the strategic authority.
Cornwall unquestionably wants those top-flight powers.
For one thing, its early adoption of devolution means it has already climbed the lower rungs.
‘National minority’
Last year, Cornwall Council passed a motion calling on the government to formally recognise the county as the fifth nation of the UK, alongside England, Scotland, Wales and Northern Ireland.
The government already accepts the Cornish have a special status in law and in 2014 they were recognised as a national minority under the European Framework Convention for the Protection of National Minorities, much like the Scots, Welsh and Irish.
The idea of a mayor is also firmly opposed by Moon and others – although some opponents of a combined authority say they might reluctantly accept a mayor if it were the price of a good deal for Cornwall alone.
Cornwall, by the by, has form when it comes to possible mayors.
Before it accepted its Level 2 deal under the Conservatives, Cornwall Council’s leadership had sought and been offered a Level 3 deal with a mayor.
Following the realisation that proposal would not command a majority in the council chamber, the plan was abandoned in favour of the less ambitious Level 2 deal.
So linking high-level devolution mayors is not a Labour novelty.
The Conservatives took the same view – but with the crucial difference that they were prepared to offer a mayor to Cornwall alone.
In his St Piran’s Day speech, Moon argued – not for the first time: “Cornwall is a mature, stable unitary authority with deep experience of strategic planning, economic development and cultural engagement.
“It must be treated as a single strategic authority with the same powers available to a mayoral combined authority.”
Cornwall’s devolution must, he says, be “bespoke” because “the Cornish are the only people in the UK with national minority status who do not yet have access to the highest levels of devolution”.
Cornish MPs Noah Law, Andrew George and Ben Maguire have made similar arguments in the Commons.
Maguire once lambasted any attempt to force Cornwall into a mayoral union with Devon as “insulting, unlawful and dangerous”.
But the government has so far stuck to its devolution rulebook. As the legislative process nears its end, nothing has really changed.
Replying to Moon in the Commons, Devolution Minister Miatta Fahnbulleh was perhaps deliberately vague.
“I look forward to continuing to work closely with our Cornwall MPs as we deliver this government’s agenda, secure the devolution deal and work together to ensure that we unlock the huge economic and local potential of this amazing part of the country,” she said.
One ministerial intervention over the course of this saga stands out.
Last November, Local Government Secretary Steve Reed sent a brief note to Cornwall Council.
“In recognition of Cornwall’s distinct local identity and history of programme delivery across the Cornwall footprint, the government is minded on an exceptional basis, to work with you to explore designating the council as a Single Foundation Strategic Authority,” he wrote.
A ‘bespoke deal’?
Were this to happen, he said it would lead to “unlocking the powers and functions available at that level of the Devolution Framework and start Cornwall on its journey to deeper and wider devolution”.
Could this be the “bespoke” deal or, at least, the first step towards it?
Some think so – but it is worth paying close attention to the language used.
A foundation authority is the basic entry-level tier of devolution in the new structure. The guidance attached to the bill is clear that that this attracts only “limited devolution”.
Essentially that is where Cornwall is now – indeed the government already describes the Devon and Torbay Combined County Authority – another Level 2 deal inherited from the Sunak era and rubber-stamped under Labour – as a foundation authority, external.
And the possibility of single authority foundation status is not as exceptional as it might sound.
In 2024, the Devolution White Paper was clear that “in exceptional circumstances the Secretary of State will have the power to designate an individual local authority as a Foundation Strategic Authority only”.
The bill guidance suggests “in rare cases, a single council which previously reached an agreement with government to access non-mayoral devolution” or “where it proved challenging for a combined authority or combined county to be established across a particular area at this stage of its devolution journey”.
Cornwall was one of a handful of councils that had negotiated single-authority devolution deals by the change of government in July 2024 and it always seemed plausible that it would be rolled over into single foundation status.
One other point about these “exceptional” single authority deals comes across loud and clear – they are not supposed to be permanent.
Going it alone
The White Paper says they will be granted “only as a stepping-stone towards forming a Mayoral Combined Authority or Mayoral Combined County Authority”, while the bill guidance describes them as an “interim” arrangement.
The only new thing here really is the indication that the government does not plan to force Cornwall into a union with Devon – though the legislation does explicitly give the secretary of state powers to impose strategic authorities and mayors “without the consent of local areas”.
But going it alone – as the legislation stands – would see Cornwall denied substantial new powers, plus the apparent expectation that it would upgrade to a mayoral combined authority at some point in the future.
Across the country as a whole, the devolution map is now largely coloured in – in principle a least.
The legislative process enshrining it all in law is also down to its last few weeks, with no indication that ministers plan to make a last-minute exception for Cornwall.
But attempts are under way to change their minds.
This week sees further debate in the House of Lords before it comes back to the Commons for the final sign-off.
Cornish Liberal Democrat peer Robin Teverson will be leading the final push for a Cornish carve-out in the Lords.
Amendments in his name would prevent areas with national minority status being forced into a combined authority or being denied top-level devolved powers, even if they refuse to accept a mayor.
‘Right direction’
However, opposition to a combined authority with Devon is not quite unanimous.
One dissenter is South East Cornwall Labour MP Anna Gelderd, whose constituency borders Devon and has economic ties.
“A Cornwall-only deal risks being left on the starting blocks as other areas race towards improvements, as we remain on the foundation-level settlement,” she said.
“On the other hand, a combined authority deal could unlock transformative funding and powers that Cornwall might not secure on its own.
“To succeed, this approach would need to ensure that Cornwall’s voice isn’t drowned out, or that resources are unfairly distributed.
“With the right safeguards, working with Devon could deliver real benefits while respecting Cornwall’s identity, history, and ensure better outcomes for residents.”
Fifteen months into this process, we should know soon whether ministers are prepared to budge.
The final word goes to Perran Moon, who claims “we’re right at the sharp end of this process now”.
He said: “We met the minister last week to go through some of the key asks… She is speaking to Cornwall Council before the end of this month and we know there are amendments coming up in the Lords.
“So I’m hopeful, I’m optimistic, but I’m not going to promise anything until there’s blood on the paper, so to speak”.