
From a correspondent:
“I just took a look at the CCG document “Devon Pre-Consultation Business Case” and found the following:
This document says that NHS England has four tests for service reconfiguration, one of which is “Clear, clinical evidence base”. This seems to come from an NHS England document “Planning, assuring and delivering service change for patients” which says the same thing and says that they are “set out in the Government Mandate to NHS England” however I cannot find anything referring to this in “The Government’s mandate to NHS England for 2016-17” and I can’t find any other similar document.
So “Clear, clinical evidence base” seems to have been made up by NHS England, which does go on to say:
“Service reconfiguration must be evidence-based and this evidence should be publicly available during the consultation and decision making stages.
A clear clinical evidence base
This ensures service reconfiguration proposals are underpinned by clear clinical evidence and align with clinical guidance and best practice. Commissioners should oversee the development of the clinical case for change, as part of the outline case. Medical directors and heads of clinical services of any providers involved can help build the clinical evidence base.”
Indeed this document could be very useful as it is some sort of blueprint for what CCGs need to do – and therefore something we can compare the CCG’s plans to.
NEW Devon CCG’s “Clear, clinical evidence base” is the following:
“The clinical evidence is clear that prolonged hospital stay increases long term physical and psychological dependence”
“The clinical evidence is clear that prolonged hospital stay increases long term physical and psychological dependence” a second time
“The Case for Change sets out clearly the evidence on gaps in existing services which we aim to address through the proposed changes. As part of this diagnostic work clinicians have undertaken a detailed review of care models for four groups of high-impact patients, who currently use significant resources in the community. This is based on identifying good practice both nationally and locally. In particular, the development of services in North Devon following development of community health and social care teams to be a single point of co-ordination for people with complex needs and a reduction in community hospital facilities”
Whilst I have not read in detail the N Devon documents that have been circulated, as far as I can tell the N Devon experience cannot genuinely to be considered to be a positive reference, and in any case the evidence linked to in the CCG documents is not “clinical evidence” but is instead a subjective survey of patients asking them whether the administration of their home visits (i.e. bookings, turning up on time) was satisfactory and says NOTHING (and I mean that in absolute terms – nada, zilch, zero, absolutely nothing) about whether the treatment was clinically effective or indeed as clinically effective as hospital care.
On page 89 there is a table which does provide some anecdotal clinical evidence, but there are no links to the underlying evidence (though we might be able to find it to verify that they have used it correctly if we search for it):
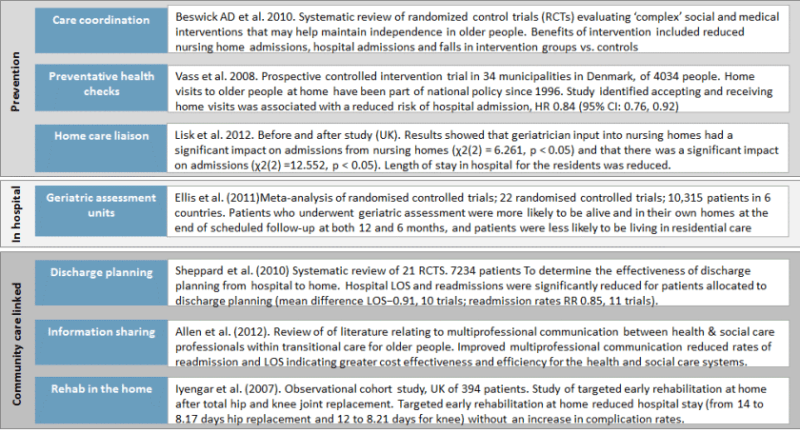
However the only evidence above directly relevant to their home-care proposals relates only to one specific type medical condition (total hip and knee replacement), and they then seem to have made a leap of faith that they can apply this to every medical condition which currently results in a stay in hospital beyond the point that hospital medical care is needed.
So it would seem that one target for “consultation feedback” is whether the CCG has met the requirements set by NHS England for a “Clear, clinical evidence base” that shows that their proposals are 1) effective and safe when considered alone, and 2) are at least as effective and safe as hospital care.
Another target for “consultation feedback” is to look at all the other areas defined by NHS England that the CCG has to meet, and see whether they have in fact done so.”
